Rottweiler, Lexi, 4 years old
CT scan of the head, native sequence, bone reconstruction
CT scan of the head, sequence after contrast administration, soft tissue reconstruction
Diagnosis
CT-Findings
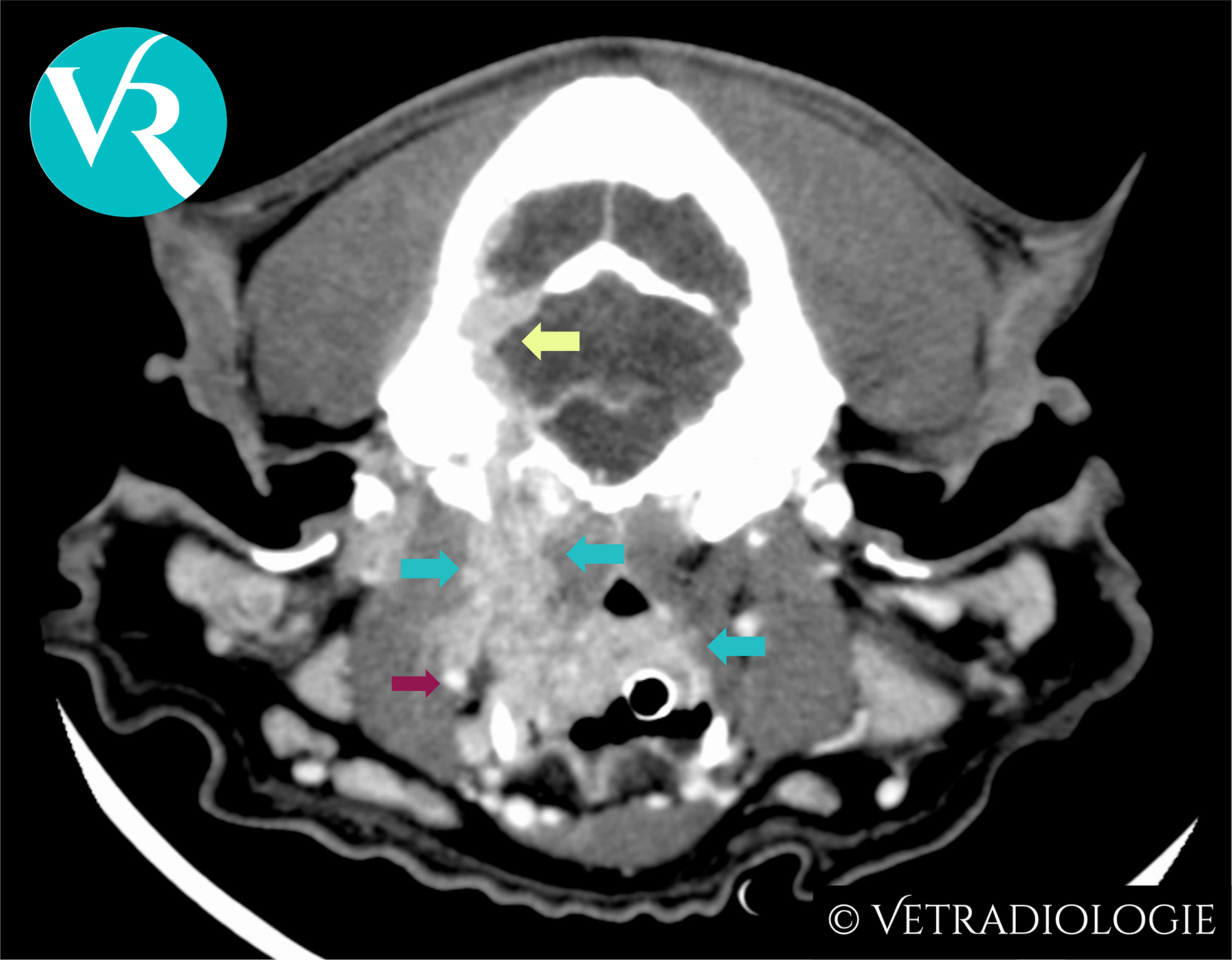
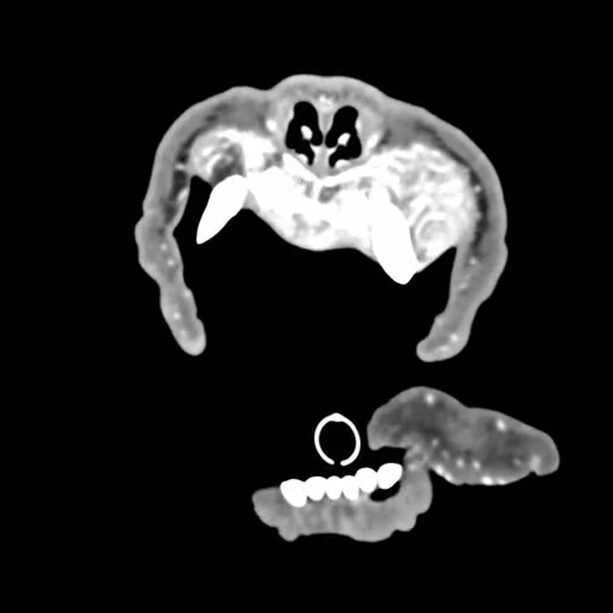
The CT scan of the head shows a complete loss of the bony structure of the maxilla and a nearly complete loss of the bony structure of the mandible. Extensive areas of osteolysis with loss of the cortical bone are visible. Both bones are highly fibrous and distended, containing hyperattenuating onion-skin-like or halo-like material that takes up contrast medium in a highly heterogeneous manner. The remaining teeth are “floating” and have no connection to bony structures.
All other skull bones, including those of both the splanchnocranium and the neurocranium, show severe osteopenia with thinning of the cortical bone, loss of the trabecular structure, and areas of osteolysis.
Note
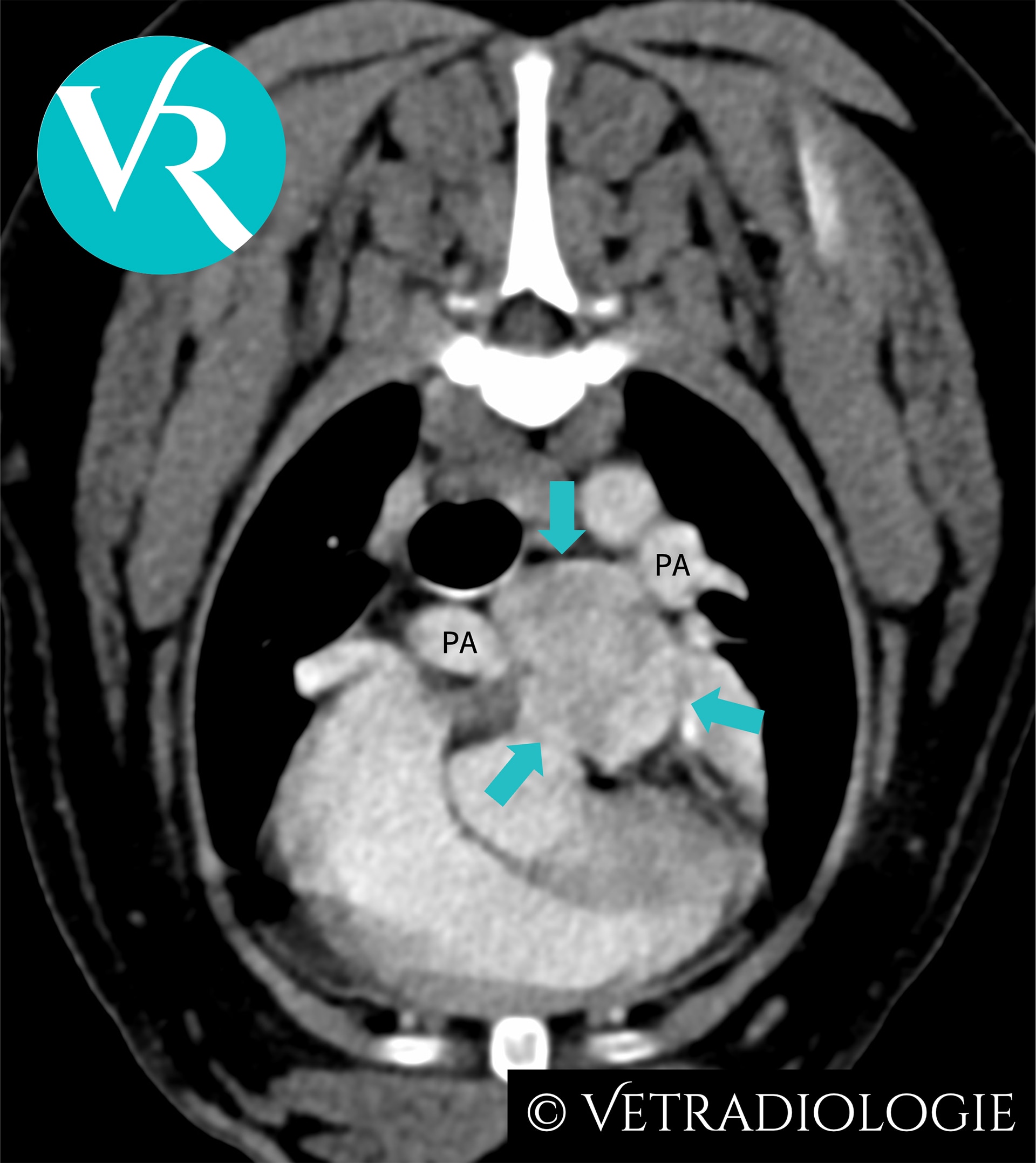
In addition to the bony changes, prominent epithelial bodies are visible on both sides of the thyroid gland. The complete CT scan also includes images of the thorax and abdomen. The kidneys appear markedly atrophic on both sides, with an irregular, nodular surface and reduced contrast enhancement. The findings in the kidneys are consistent with bilateral atrophic kidneys (nephrocirrhosis).
CT-Diagnosis
- Severe fibrous osteodystrophy (rubber jaw syndrome)
- Severe osteopenia of the facial skeleton and neurocranium
- Generalized enlargement of the parathyroid glands
- Bilateral kidney atrophy (nephrocirrhosis)
Discussion
The CT scan findings of “Lexi’s” head show the consequences of secondary renal hyperparathyroidism, including advanced generalized osteopenia of the skull bones and what is known as fibrous osteodystrophy of the jaw bones (rubber jaw osteodystrophy). Fibrous osteodystrophy is a metabolic bone disease in which increased bone resorption and its replacement by collagenous connective tissue lead to reduced bone density (osteopenia).
The cause is a prolonged elevation of parathyroid hormone levels in the blood, which results in the following pleiotropic effects:
| Effect on the bones | Effects on the kidneys | Effect on the intestines |
|---|---|---|
|
|
|
|
This hyperparathyroidism can be primary (endocrine-active hyperplasia, adenomas, or adenocarcinomas of the parathyroid gland), secondary to renal disease (resulting from chronic kidney disease), or tertiary (continuously high PTH secretion in the course of secondary hyperparathyroidism that is no longer subject to normal regulatory mechanisms).
In Lexi’s case, the atrophic kidneys and azotemia indicate the presence of chronic renal insufficiency. Lexi’s enlarged parathyroid glands respond to the resulting hyperphosphatemia and hypocalcemia by overproducing parathyroid hormone, which in turn causes a severe disturbance in calcium homeostasis (renal hyperparathyroidism).
References
- Baumgärtner, W., Ulrich, R. (2020). Osteodystrophia fibrosa. In: Baumgärtner W, Gruber A, Hrsg. Spezielle Pathologie für die Tiermedizin (2., aktualisierte Auflage). Stuttgart: Thieme.
- Brachthäuser, L., Pingen, C. H., Hecht, W., Reinacher, M. (2013). Rubber jaw in a Weimaraner dog due to juvenile nephropathy. A case without evidence for genetic involvement. Tierärztliche Praxis Ausgabe K: Kleintiere / Heimtiere, 41(3), 198–202.
- Grünberg, W., Ramirez, A. (2020). Fibrous Osteodystrophy in Animals. MSD Veterinary Manual. https://www.msdvetmanual.com/musculoskeletal-system/dystrophies-associated-with-calcium-phosphorus-and-vitamin-d/fibrous-osteodystrophy-in-animals
- Kyle, M. G., Davis, G. B., Thompson, K. G. (1985). Renal osteodystrophy with facial hyperostosis and ‘rubber jaw’ in an adult dog. New Zealand Veterinary Journal, 33(7), 118–120.
- Waller, S. B., Correia Canuto, F. J., Correia Costa, P. P., Louzada Dias Cavalcanti, E. A. N., de Oliveira Cavalcanti, G. A., Vasconcelos, M., & Blum Cleff, M. (2019). Maxillomandibular Deformity in a Canine with Fibrous Osteodystrophy Secondary to Chronic Kidney Disease. Acta Scientiae Veterinariae, 47 (Suppl 1).