Portosystemic shunts
Congential portosystemic shunts
Which types of portosystemic shunts (PSS) do we differentiate?
Is there an easy way to memorize the classical types of PSS in the dog?
In the following I will try to explain this complex topic.

Generally said:
- Small breed dog = extrahepatic
- Large breed dog = intrahepatic
Below you find a short guide to the different types of PSSs and the classification of congenital PSS. The following points should be addressed:
- Number of shunt vessels
- Insertion of the shunt vessel
- Origin of the shunt vessels
Additionally it is helpful to remember which PSS is common.
Intrahepatic PSS – Classification
Number
- Single PSS
- Multiple PSS
Insertion
Intrahepatic PSS always insert into a hepatic vein and therefore finally the caudal vena cava.
Origin / Course
Right divisional PSS
- Origin: right intrahepatic branch
- Course: Lobus hepatis dexter lateralis and Lobus caudatus
Central divisional PSS
- Origin: right intrahepatic branch
- Course: Lobus hepatis dexter medialis and Lobus quadratus
Left divisional PSS
- Origin: left intraheptic branch = persistent Ductus venosus
- Course: Lobus hepatis sinister medialis and Lobus quadratus
Incidence
Common:
- Right divisional intrahepatic PSS
- Left divisional intrahepatic PSS
Uncommon / rare:
- Central divisional PSS
- Multiple congenital intrahepatic PSS
- Venovenous collaterals
Extrahepatic PSS – Classification
Number
Congenital, extrahepatic PSSs always have a single vessel! Multiple extrahepatic PSS are always acquired!
Insertion
Porto-caval
- Insertion: Caudal vena cava
Porto-azygos
- Insertion: Azygos vein
Porto-phrenic
- Insertion: Hepatic vein or caudal vena cava at the level of the diaphragm
Porto-renal
- Insertion: Left renal vein
Origin / Course
Splenic vein or left gastric vein
- Can be found in: porto-caval, porto-azygos and porto-phrenic PSSs (origin in right gastric vein is possible but uncommon)
Gastroduodenal vein:
- Can be found in: porto-caval PSS
Right gastric vein
- Can be found in: porto-phrenic PSS
Cranial mesenteric vein (possibly origin of portal vein)
- Can be found in: porto-renal PSS
Incidence
Common:
- Porto-caval PSS with origin in the gastroduodenal vein or splenic vein
- Porto-azygos PSS with origin in the splenic vein
- Porto-phrenic PSS with origin in the splenic vein
Uncommon / rare:
- Porto-renal PSS
- Other
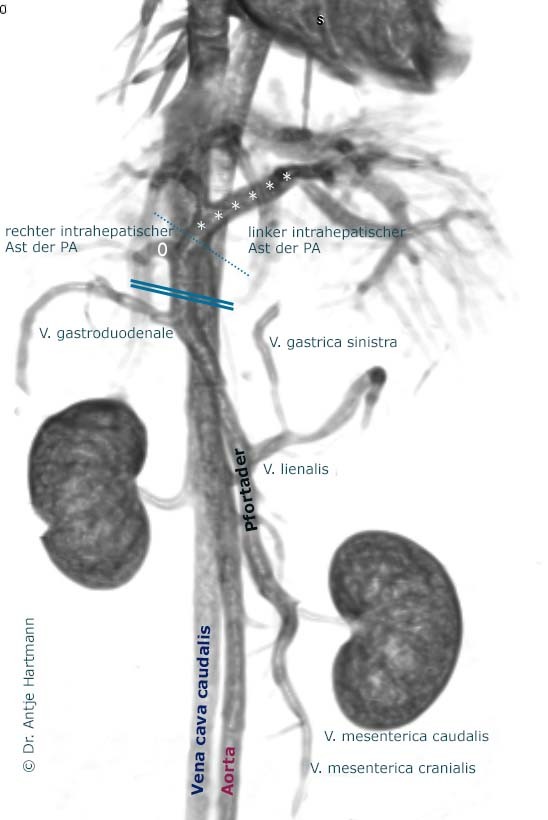
To be able to identify the form of PSS you are dealing with it is helpful to remember the normal anatomy of the portal vein.
The portal vein is entering the liver slightly more to the right side. Looking at its intrahepatic branching pattern: after entering the liver a small right branch is coming off the portal vein. It supplies the right lateral hepatic lobe and the caudate process of the caudate lobe. The remaining and therefor largest portion of the liver is supplied by the left intrahepatic branch of the portal vein.
Brief and easy:
- The right intrahepatic branch is small and short.
- The left intrahepatic branch is long.
Therefore intrahepatic PSS arising from the
- right branch create a short loop.
- left branch create a long loop.
But how can you differentiate a central divisional intrahepatic PSS from a right divisional intrahepatic PSS?
First it is helpful to remember that central divisional PSSs are rare. Therefore it is more likely to have a right divisional intrahepatic PSS. Additionally:
The central divisional intrahepatic PSS has a very short loop resembling a foramen more than an actual, loop; in contrast the right divisional intrahepatic PSS shows a short loop. Thus it can be said: for the extrahepatic porto-caval PSSs the opposite of intrahepatic PSSs is true.
- The right extrahepatic PSS is long.
- The left extrahepatic PSS is short.
Porto-azygos PSSs are the only PSSs in which you can see a vessel coursing dorsally. Additionally the azygos vein is enlarged and easily visible cranial to the shunt.
Porto-phrenic PSSs arise caudal to the liver, running in a large curve along the left side of the liver (rarely the right side) towards the diaphragm. The insertion is immediately caudal to the diaphragm and appears to lie within the hepatic parenchyma.