French Bulldog, Sammy, 9 years
CT dated September 2021. Presented with 10d history of cough, dyspnea and nasal discharge. Acute right-sided facial paralysis and lethargy.
Diagnosis
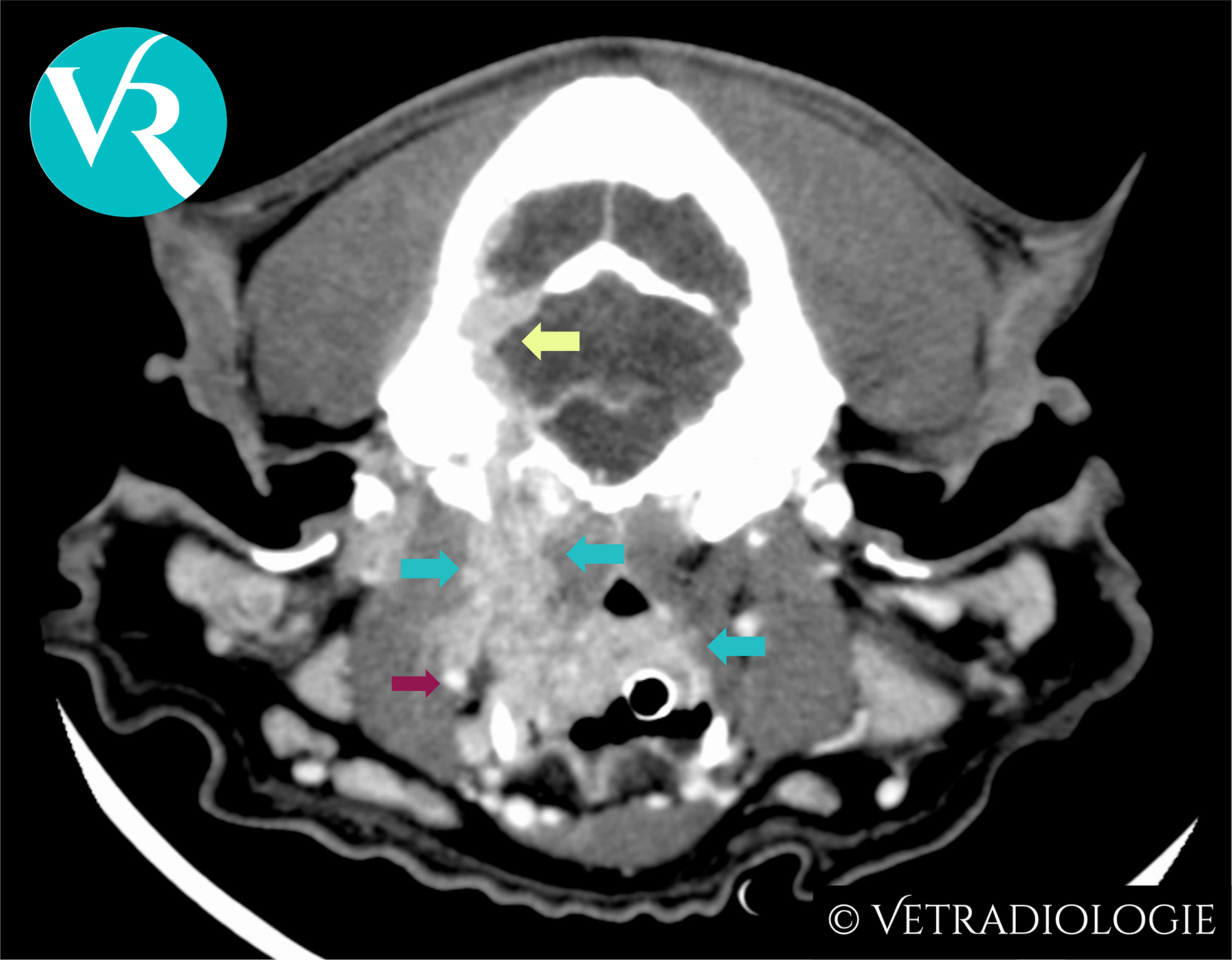
Sammy’s CT-Study: Infiltrative soft tissue mass (turquoise arrows) exhibiting marked heterogeneous contrast enhancement and invasion of the cranial vault (yellow arrow) along the plane of the right internal carotid artery (red arrow).
CT-Findings
Right-sided retropharyngeal soft tissue mass located medial to the right mandibular salivary gland in the region of the common carotid arterial bifurcation, with craniodorsal mass extension towards the cranial vault. There is associated invasion of the digastric and medial pterygoid muscles, and osteolysis of the right temporal bone (including petrous, tympanic and squamous parts). There is extension of the lesion into the caudal fossa via moth-eaten and permeative osteolysis of the squamous part of the right temporal bone, with the intracranial mass component reaching and conforming to the tentorium cerebelli ventrally.
Caudally, the lesion extends along the right common carotid artery to the approximate level of the thyroid gland.
The lesion exhibits marked, heterogeneous contrast enhancement.
CT-Diagnosis
- Aggressive, invasive soft tissue mass originating near the bifurcation of the right common carotid artery.
Discussion
The imaging features of the mass are consistent with a carotid body tumor/glomus caroticum tumor. This subtype of paraganglioma belongs to the group of neuroendocrine tumors (NETs).
Brachycephalic dog breeds are predisposed.
Carotid body tumors arise from the neuroendocrine chemoreceptors of the carotid glomus, located at the bifurcation of the common carotid artery. Similar clusters of chemoreceptors (glomera) exist in the wall of the aorta (aortic body glomus) and the pulmonary trunk (pulmonary glomus), where tumor development (chemodectomas, glomus aorticum tumors) has likewise been described.
As circulatory regulatory structures, the chemoreceptors of the glomera respond to reduced oxygen partial pressure and to changes in blood pH.
Chronic hypoxia and respiratory acidosis associated with brachycephalic obstructive airway syndrome (BOAS) lead to persistent stimulation of these chemoreceptors. It is assumed that this—either alone or in combination with a genetic component—accounts for the described breed predisposition to the development of carotid body tumors and chemodectomas.
The clinical presentation varies depending on tumor size and the extent of involvement of adjacent structures. Potential symptoms include regional discomfort, head tilt, coughing, dyspnea, Horner’s syndrome, or dysphagia.
On CT, carotid body tumors appear as highly vascularized, locally invasive masses with marked, heterogeneous contrast enhancement.
References
- Buscaglia NA, Johnson PJ. What Is Your Diagnosis? J Am Vet Med Assoc. 2019;254(4):467-469. doi:10.2460/javma.254.4.467.
- Crawford-Jennings MI, Chavez LD, Loessberg ER, Carvallo-Chaigneau FR. Aortic body tumor with intracardiac metastasis in a dog. J Vet Diagn Invest. 2025 Mar;37(2):345-348. doi: 10.1177/10406387241304438.
- Fife W, Mattoon J, Drost WT, Groppe D, Wellman M. Imaging features of a presumed carotid body tumor in a dog. Vet Radiol Ultrasound. 2003;44(3):322-325. doi:10.1111/j.1740-8261.2003.tb00463.
- Kromhout K, Gielen I, De Cock HE, et al. Magnetic resonance and computed tomography imaging of a carotid body tumor in a dog. Acta Vet Scand. 2012;54:24. doi:10.1186/1751-0147-54-24.
- Mai W, Seiler GS, Lindl-Bylicki BJ, et al. CT and MRI features of carotid body paragangliomas in 16 dogs. Vet Radiol Ultrasound. 2015;56:374-383. doi:10.1111/vru.12251.
- Obradovich JE, Withrow SJ, Powers BE, Walshaw R. Carotid body tumors in the dog. Eleven cases (1978–1988). J Vet Intern Med. 1992;6(2):96-101. doi:10.1111/j.1939-1676.1992.tb03158.
- Wess G. Kardiale und perikardiale Tumoren. In: Kessler M, Hrsg. Kleintieronkologie. 4., vollständig überarbeitete Auflage. Stuttgart: Thieme; 2022:600f.