Cardiac diseases
An accurate diagnosis regarding the type of cardiac disease is generally not made on radiographs alone. However, radiographs do contain more information than just: “cardiomegaly” and “pulmonary oedema” present / not present.
Careful evaluation of the cardiac silhouette on radiographs usually allows narrowing down the list of differential diagnoses to at least two, and sometimes even to a final diagnosis.
Normal anatomy — the clock face analogy
For an accurate assessment of the cardiac silhouette, knowledge of the normal cardiac anatomy it essential; that is where the clock face analogy comes in. The clock face is projected onto the cardiac silhouette on the DV/VD view and helps relate enlargement of outflow tracts and cardiac chambers to a particular time on the clock. The same principle can be applied to the lateral views.
Clock face analogy — dog
Abbreviations used:
Ao=aorta, LA= left atrium, LAu= left auricular appendage, MPA= main pulmonary artery segment, PA=pulmonary artery, PV= pulmonary vein, RA= right atrium; RAu= right auricular appendage; RV= right ventricle. The numbers indicate the “time” in which the named structures can be found.
Click on an image to enlarge it.

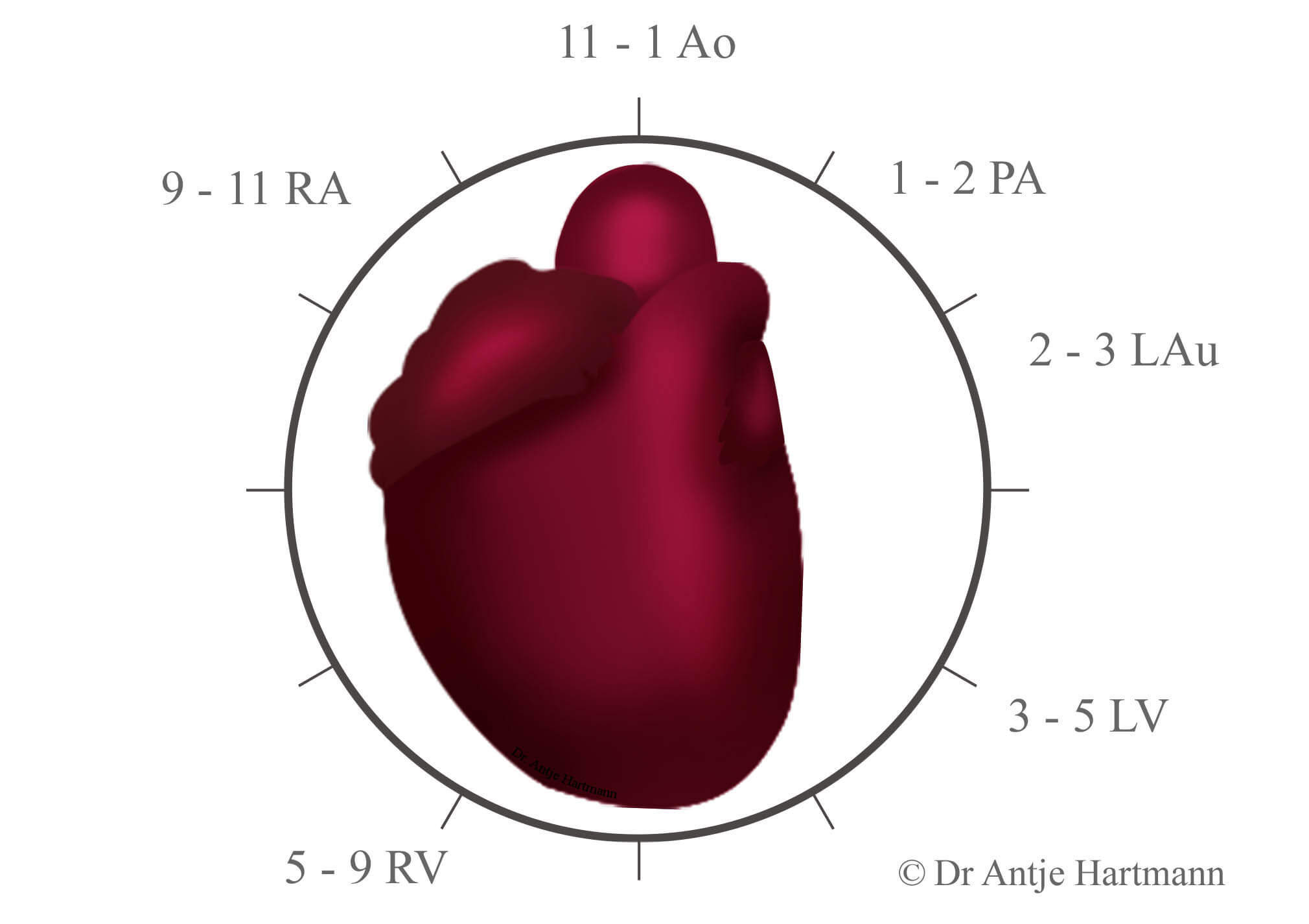
The LA is not visible on a VD/DV view. It is located dorsal to the cardiac silhouette, level with the carina and between the two main stem bronchi. Enlargement of the LA will result in splaying of the main stem bronchi and lateral displacement of the LAu appendage between 2 and 3 o’clock.
Clock face analogy — cat
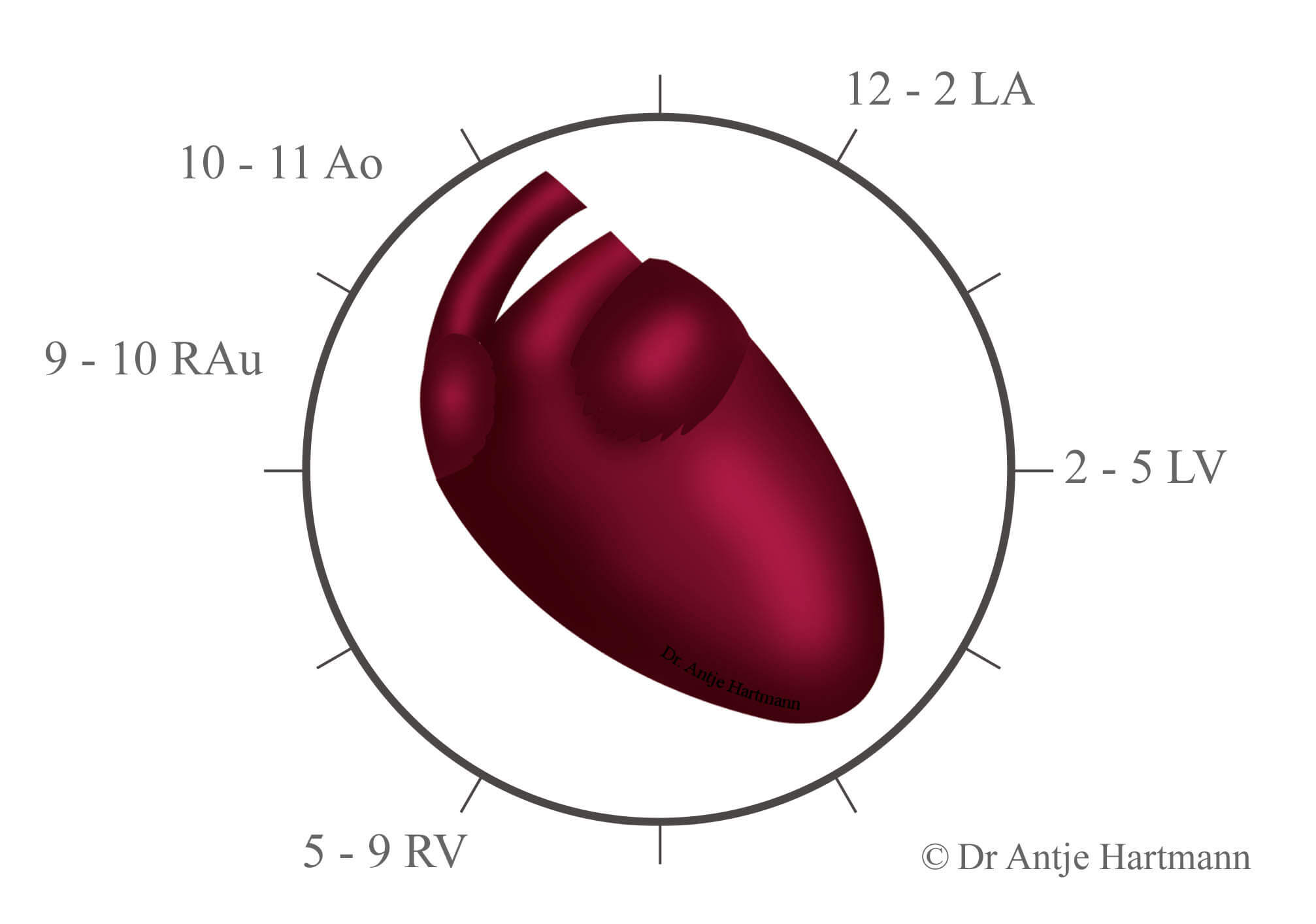
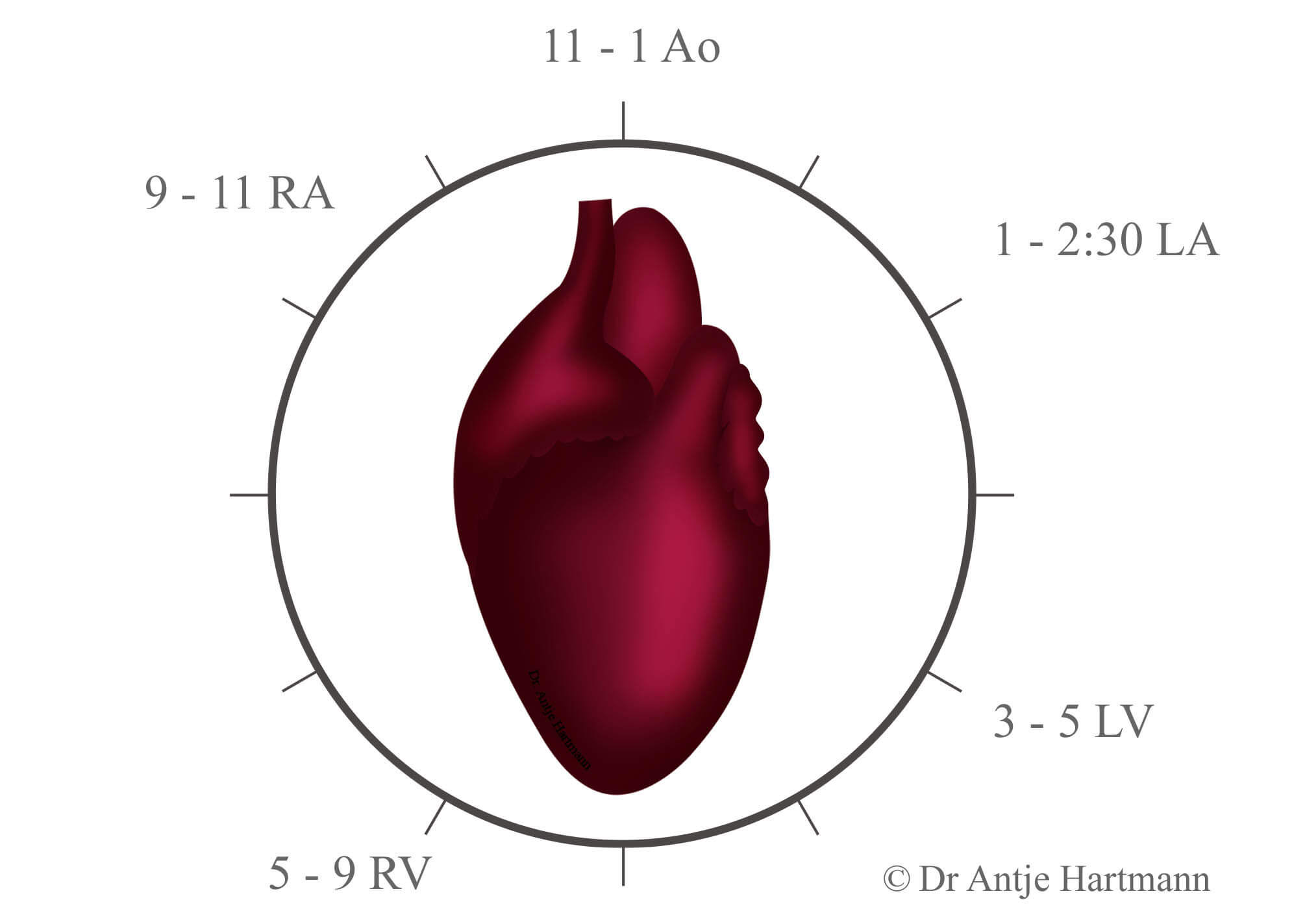
Contrary to the dog, the LA is located between 1 and 2:30 o’clock on the DV/VD view. Enlargement leads to the typical “Valentine shape” of the heart in hypertrophic cardiomyopathy. The MPA does not form part of the outer cardiac silhouette but is superimposed onto the heart.
As a rule of thumb:
- Is the cardiac silhouette too tall, the L heart is enlarged
- Is the cardiac silhouette too wide, the R heart is enlarged
To allow narrowing down the list of differential diagnoses, an attempt should be made to identify which particular part of the heart is enlarged (clock face!).
- Is a left- or right sided cardiac enlargement more likely due to an enlargement of the chamber, atrium or both of them?
- How does the main pulmonary artery appear? Is it also enlarged?
Finally pulmonary vessel, CVC as well as the cranial abdomen should be assessed.
- Do the pulmonary vessels have a normal diameter; are they enlarged or smaller than normal?
- Are pulmonary arteries, pulmonary veins or are both affected?
- Is pulmonary oedema present?
- Is the CVC enlarged?
- Does the liver protrude beyond the costal arch?
- Is there ascites?
The following section lists possible diseases which may cause enlargement of particular areas of the heart and is divided into congenital and acquired anomalies.
Diseases which show the word “rare” hardly ever lead to enlargement of a particular cardiac component; the term “occasional” indicates enlargement of a particular cardiac component every now and then. These diseases either result in enlargement of a different part of the heart or they do not result in radiographically evidence of cardiac enlargement. In case they do show enlargement of a different part of the heart, enlargement of the particular chamber or outflow tract is referred to as “rare” or “occasional” when it occurs at a later stage.
Supplementary information is given regarding concomitant changes related to heart and lung. These are subdivided into changes which have to be present (“must”) and changes which may be present (“possible”) in connection with the disease mentioned.
Further information relating to specific diseases can be found under “congenital cardiac abnormalities” and “acquired cardiac abnormalities”.
Enlargement of the L atrium
Congenital anomalies
Mitral dysplasia
- concomitant changes (possible)
-
- Enlarged pulmonary veins (PV)
- Pulmonary oedema
PDA
- concomitant changes
-
- segmental aortic dilatation (aortic knuckle/bump) (must)
- Pulmonary hyperperfusion with enlargement of PA and PV (must)
- LV enlargement (possible)
- Enlargement of aortic arch (possible)
- Enlargement MPA (possible)
- Enlargement LAu (possible)
Aortic stenosis (occasional)
- concomitant changes
-
- LV enlargement (must)
- Dilatation of ascending aorta (possible)
Mitral stenosis (rare)
- concomitant changes (possible)
-
- Congestion PV
- Pulmonary oedema
- In case of pulmonary hypertension due to Eisenmenger Syndrome enlargement of RV and RA
Persistent atrio-venticular (AV) canal
- concomitant changes (possible)
-
- RA enlargement
- MPA enlargement
- RV enlargement
Cor atrium sinister
- concomitant changes (possible)
-
- Pulmonary oedema
VSD (rare)
- concomitant changes (possible)
-
- LV enlargement
- MPA enlargement
- Pulmonary hyperperfusion
- RV enlargement
Acquired diseases
Degenerative mitral valve disease / mitral endocardiosis
- concomitant changes (possible)
-
- LV enlargement
- PV distension
- Pulmonary oedema (during decompensation)
Dilated cardiomyopathy
- concomitant changes
-
- LV enlargement (must)
- RA enlargement (possible)
- RV enlargement (possible)
Hypertrophic cardiomyopathy (HCM) & restrictive cardiomyopathy (RCM)
- concomitant changes (possible)
-
- LV enlargement
- Pulmonary hyperperfusion
- Pulmonary oedema
Systemic hypertension
- concomitant changes (possible)
-
- Pulmonary hyperperfusion
- Pulmonary oedema
Enlargement of the L ventricle
Congenital anomalies
(Sub-) aortic stenosis
- concomitant changes (possible)
-
- LA enlargement
- Dilatation of ascending aorta
PDA
- concomitant changes
-
- segmental dilatation descending aorta (aortic knuckle/bump) (must)
- Pulmonary hyperperfusion with enlargement of PA and PV (must)
- LA enlargement (possible)
- Enlargement of aortic arch (possible)
- Enlargement MPA (possible)
- Enlargement LAu (possible)
Mitral dysplasia
- concomitant changes
-
- LA enlargement (must)
VSD (rare)
- concomitant changes (possible)
-
- LA enlargement
- MPA enlargement
- Pulmonary hyperperfusion
- RV enlargement
Acquired diseases
Degenerative mitral valve disease / mitral endocardiosis
- concomitant changes
-
- LA enlargement (must)
- PV enlarged (possible)
- Pulmonary oedema (possible during decompensation)
Dilated cardiomyopathy
- concomitant changes
-
- LA enlargement (must)
- RA enlargement (possible)
- RV enlargement (possible)
HCM
- concomitant changes
-
- LA enlargement (must)
- Pulmonary hyperperfusion (possible)
- Pulmonary oedema (possible)
Enlargement of the R atrium
Congenital anomalies
Tricuspid dysplasia
- concomitant changes (possible)
-
- Wide CVC
- Ascites
Pulmonic stenosis (occasional)
- concomitant changes (must)
-
- MPA enlargement
- RV enlargement
- Pulmonary hypoperfusion
Atrium septal defect (rare, only in late stage of the disease)
- concomitant changes
-
- RV enlargement (must)
- MPA enlargement (possible)
- Pulmonary hyperperfusion (possible)
Persistent atrio-venticular (AV) canal
- concomitant changes (possible)
-
- RV enlargement
- MPA enlargement
- LA enlargement
Cor triatrium dexter
- Wide CVC
Tricuspid valve stenosis (rare)
- concomitant changes (possible)
-
- Wide CVC
- Hepatomegaly
- Ascites
Acquired diseases
Dilated cardiomy0pathy
- concomitant changes (must)
-
- LV enlargement
- LA enlargement
- RV enlargement
Degenerative tricuspid valve disease/ tricuspid valve endocardiosis
- concomitant changes (possible)
-
- RV enlargement
Cor pulmonale / pulmonary hypertension
- concomitant changes (must)
-
- RV enlargement
- MPA enlargement
Heartworm disease/Dirofilariasis
- concomitant changes (must)
-
- MPA enlargement
- Widening of the central portion of the pulmonary artery (PA), tortuous path, potential abrupt luminal changes (esp. in the caudal lobe)
Arythmogenic R ventricular cardiomyopathy (cat)
- concomitant changes (possible)
-
- congestion CVC and ascites
- RV enlargement
Hypertrophic cardiomyopathy (HCM)/restrictive cardiomyopathy (RCM)
Both diseases can mimic RA enlargement. Due to the severely enlarged LA the RA is displaced laterally so that the R cardiac silhouette shows a knuckle at 11o’clock.
Enlargement of the R ventricle
Congenital anomalies
Pulmonic stenosis concomitant
- changes
-
- MPA enlargement (must)
- RA enlargement (possible)
- Pulmonary hypoperfusion (possible)
Tricuspid dysplasia
- concomitant changes (must)
-
- RA enlargement
Atrial-septal defect (rare, only with chronicity)
- concomitant changes (possible)
-
- RA enlargement
- MPA enlargement
- Pulmonary hyperperfusion
Reversed patent ductus arteriosus (PDA)
- concomitant changes (possible)
-
- MPA enlargement
- In case of shunt reversal also LV+LA enlargement and aortic knuckle at 1 o’clock
Tetralogy of Fallot (rare, radiographs generally NAD)
- concomitant changes (possible)
-
- Pulmonary hypoperfusion
Persistent atrio-venticular (AV) canal
- concomitant changes (possible)
-
- RA enlargement
- MPA enlargement
- LA enlargement
Ventricular septal defect (VSD) (rare)
- concomitant changes (possible)
-
- LA enlargement (more likely than RA enlargement)
- LV enlargement (more likely than RV enlargement)
- MPA enlargement
- Pulmonary hyperperfusion
Acquired diseases
Dilated cardiomyopathy
- concomitant changes
-
- LV enlargement (must)
- LA enlargement (must)
- RA enlargement (possible)
Arrythmogenic R ventricular cardiomyopathy (cat)
- concomitant changes (possible)
-
- RA enlargement
- Wide CVC
Cor pulmonale / pulmonary hypertension
- concomitant changes
-
- MPA enlargement (must)
- RA enlargement (possible)
Degenerative tricuspid valve disease/ tricuspid valve endocardiosis
- concomitant changes (must)
-
- RA enlargement